A lot of information is enciphered in heart sound. There are two main problems: it is difficult to perceive this sound because it is too faint, and it is not simple to interpret reaped information. The later is some kind of understanding a foreign language. Let us continue our talk about the language of the heart.
While listening to S1, it is important to note:
- the loudness of S1
- the interval of the splitting of S1
- sounds just before and after S1
Let us talk about loudness. This characteristic is helpful while examining every patient.
In most of the cases, this simple rule is useful: the shorter PR-interval, the louder S1. Plus: mitral stenosis of any aetiology makes S1 loud.
Why?
Because the intensity of S1 depends on the position of cusps of mitral and tricuspid valves at the beginning of systole. Left and right ventricular pressure rises not linearly, but rather exponentially as you can see on the picture below. It rises slowly at the beginning and quickly at the end. If atrioventricular valves close later, they close with greater velocity. If these valves are wide opened, then later they close with greater velocity.
If PR-interval is short, then mitral and tricuspid valves are wide opened at the beginning of systole. And vice versa.
Listen to a patient with short PR-interval (0.12 sec) and loud S1:
Now with long PR-interval (0.2 sec) and faint S1. This is a pregnant woman in her thirtieth, normal third heart sound is heard.
Now listen to a male patient in his seventieth with third-degree AV block. PR-interval changes every heartbeat which leads to the alternation of S1' intensity. Pansystolic band-like murmur is also present.
Mitral stenosis causes pressure's elevation in the left atrium which postpones mitral valves closure. That is why it closes with greater velocity and loudness.
Now listen to the next patient with mitral stenosis and mild aortic regurgitation. Use headphones. Note (look at the sonogram below):
- very loud S1
- soft S2
- a faint decrescendo high-frequency murmur of aortic regurgitation started with S2
- a faint low-frequency mid-diastolic rumble of mitral stenosis
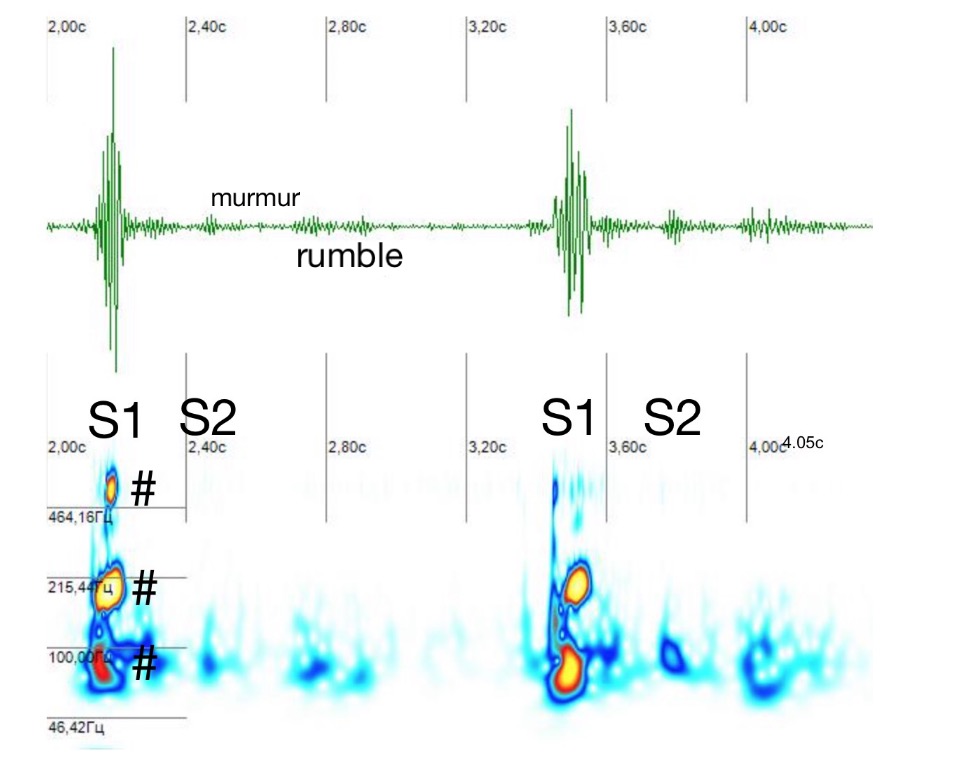
S1 containes three harmonics #. These harmonics give to S1 musical quality.
The cause of mitral stenosis does not matter. Left atrial myxoma is a rare case of mitral stenosis and leads to loud S1. Here is a typical case.