There are two kinds of problems in heart auscultation:
- an auscultatory sign can be faint
- an auscultatory picture can be too complex
By the way, I am going to publish the book about solutions of such problems.
Here I am going to describe a case with very faint and rare musical murmur which was very difficult to hear.
A young man... well, the whole story doesn't matter. Listen between the apex and left the lower sternal border, the patient is on left decubitus position:
S1 is relatively faint; S2 has average intensity. There is very soft short early diastolic murmur somewhere on the threshold of audibility. Use headphones and try to hear this murmur.
Any diastolic murmur can not be functional. What is the cause?
There are only two valvular lesions which can cause diastolic murmur:
- mitral or tricuspid stenosis
- aortic or pulmonary regurgitation
But these pathologies produce different murmurs. Mitral and tricuspid stenosis produce low frequency (never high frequency!) murmurs. Aortic and pulmonary regurgitations produce prolonged decrescendo murmurs just after S2 without pause.
Here we have short high-frequency musical murmur in the early diastole. There is a short interval between S2 and the beginning of the murmur. This is a very unusual finding!
I hypothesised that the cause of the murmur was a false tendon attached in the left ventricle perpendicularly to diastolic inflow. I performed an Echo and found this chorda on its place. My colleges were impressed, but this is not the main topic of this post.
By the way, such chordae are common findings, but such murmurs are not.
Ok. I understand, that this murmur is not easily heard. It is bloody hard to hear it. Especially without headphones. In such cases I frequently think: are there any sound at all? Or it only seemed to me?
I decided to prove the existence this murmur. There are two ways to do that:
- to visualise it
- to make it louder and noticeable
It is not possible to visualise faint high-frequency sounds because our hearing ability in this diapason is mutch more accurate than the sensitivity of visualising software.
I decided to make this murmur louder. To achieve this, I increased all high frequencies and attenuated low frequencies by the equaliser. I obtained this:
Its visualisation is below:
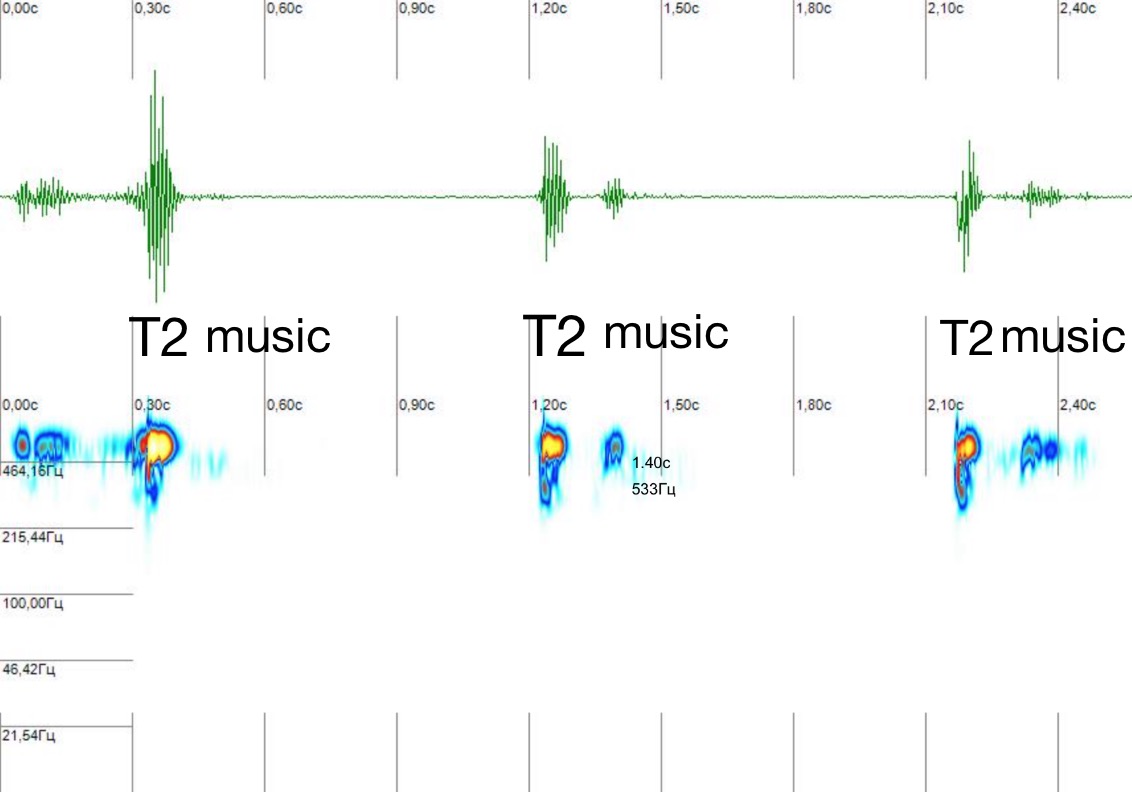
The oscillatory conventional phonocardiogram is above; spectrogram is below. S1 is absent because it has gone with removed low frequencies. After loud S2 short musical murmur 'music' with intermittent loudness is present.
Finally, I decided to cut out everything from the recording except the murmur. Listen to the musical murmur alone; any other sounds was removed. The loudness of the murmur was significantly increased.
Key points to learn:
Contrary to some systolic murmur, diastolic murmurs are never functional and have an anatomic cause.
I described a rare case of diastolic murmur associated with the left ventricular false tendon. This murmur is innocent in fact.